
Compartmental models are often used to simplify the mathematical modeling of infectious disease. The population is split into compartments and it is assumed each individual in a compartment has the same characteristics. While this may appear to be rather crude, such models have shown to accurately model previous infectious outbreaks[1].
We start with the following set of non-linear first-order differential equations:







where we have made the following compartments: susceptible ( ), exposed (
), exposed ( ), infectious (
), infectious ( ), recovered (
), recovered ( ) and dead (
) and dead ( ) and
) and  is time (say in units of days).
is time (say in units of days).  is the transmission rate of infection while
is the transmission rate of infection while  represent the transmission rate of infection from exposed individuals who have yet to displayed any symptoms.
represent the transmission rate of infection from exposed individuals who have yet to displayed any symptoms.  (
( is the mean latent period) is the rate of exposed to infections state. Similarly,
is the mean latent period) is the rate of exposed to infections state. Similarly,  is the rate of recovery while
is the rate of recovery while  is the rate of death. If the total case fatality proportion (CFP) is known, then
is the rate of death. If the total case fatality proportion (CFP) is known, then  . We implicitly assume that any recovered individuals are now immune. This may not be the case.
. We implicitly assume that any recovered individuals are now immune. This may not be the case.
This simple model can be expanded to include sub-compartments, say,  where
where  could represent different slices of population demographics or it could represent different geographic locations and then a network could be included to show how the different mix together. We ignore such models since they require more information than is currently available. We further ignore the natural birth and death rates of the general population, implicitly assuming the infectious outbreak would not disturb the equilibrium natural birth and death rates (this may not be realistic for the latter).
could represent different slices of population demographics or it could represent different geographic locations and then a network could be included to show how the different mix together. We ignore such models since they require more information than is currently available. We further ignore the natural birth and death rates of the general population, implicitly assuming the infectious outbreak would not disturb the equilibrium natural birth and death rates (this may not be realistic for the latter).
We will simplify the model further. In the current case, most evidence suggests exposed individuals are infectious (i.e.  ), so there is no real difference between and . By making this assumptions, we eliminate some time delay between being exposed and infected individuals showing symptoms (useful for predicting temporal demands on the healthcare system). With this assumption, we can set to a large value and get a set of simplified equations:
), so there is no real difference between and . By making this assumptions, we eliminate some time delay between being exposed and infected individuals showing symptoms (useful for predicting temporal demands on the healthcare system). With this assumption, we can set to a large value and get a set of simplified equations:




We see that susceptible individuals enter infectious state at a rate  . That is,
. That is,  represents the probability of a random contact between an infectious and susceptible individuals.
represents the probability of a random contact between an infectious and susceptible individuals.
To stop the increase of rate of new of infections ( 0), we immediately see
0), we immediately see
 or
or 
would represent either no infectious people or infectious people not mixing with susceptible population (i.e. quarantined). Otherwise we see that the ratio of susceptible individuals to the population ( ) must balance
) must balance  , where
, where  is the basic reproduction number. For comparison is 12-18 for measles, 3.5-6 for smallpox, 2-5 for HIV, 1.4-2.8 for Spanish Flu and 0.9-2.1 for typical influenza. Preliminary data suggests is between 1.4 and 3.9 for COVID-19. Assuming
is the basic reproduction number. For comparison is 12-18 for measles, 3.5-6 for smallpox, 2-5 for HIV, 1.4-2.8 for Spanish Flu and 0.9-2.1 for typical influenza. Preliminary data suggests is between 1.4 and 3.9 for COVID-19. Assuming  ,
,

Therefore, to stop the increase of new infections,  40%. In other words, over 60% of the population will become infected before the rate of new infections has stopped increasing. Unfortunately, this only represents the peak in infections. There will be additional infections (though with diminishing rates) until the rate falls to zero.
40%. In other words, over 60% of the population will become infected before the rate of new infections has stopped increasing. Unfortunately, this only represents the peak in infections. There will be additional infections (though with diminishing rates) until the rate falls to zero.
To find the cumulative number of infections ( ), one needs to solve the coupled non-linear differential equations. These equations do not have (non-trivial) analytic solutions and so numerical modeling is required.
), one needs to solve the coupled non-linear differential equations. These equations do not have (non-trivial) analytic solutions and so numerical modeling is required.
Using Mathematica, we can set up the equations as
qq = NDSolve[{
beta[t] == beta0,
n[t] == s[t] + i[t] + r[t],
s'[t] == -beta[t] s[t] i[t] / n[t],
i'[t] == beta[t] s[t] i[t] / n[t] - (delta + gamma) i[t],
r'[t] == gamma i[t],
d'[t] == delta i[t],
c'[t] == beta[t] s[t] i[t] / n[t],
i[0] == 0.0001, s[0] == 1.0 - i[0], r[0] == 0, d[0] == 0, c[0] == 0}
/. beta0 -> r0 (delta + gamma) /. delta -> gamma cfp/(1 - cfp)
/. gamma -> 1/11 /. cfp -> .0011 /. r0 -> 2.5,
{s, i, r, d, c}, {t, 200 (*6.6months*)}]
where , CFP = 1.1%, mean time to recovery ( ) is 11 days and , , , and
) is 11 days and , , , and  are interpreted as the fraction of the initial population
are interpreted as the fraction of the initial population  . We set 0.01% of the population to be infected with the rest susceptible. The follow Mathematica code will plot infections and cumulative infections:
. We set 0.01% of the population to be infected with the rest susceptible. The follow Mathematica code will plot infections and cumulative infections:
Plot[Evaluate[{i[t],c[t]} /. qq], {t, 0, 150},
PlotLegends -> (Style[#, Black, Bold, 18] & /@ {"infections", "cumulative infections"}),
AxesLabel -> {Style["days", Black, 18]}, TicksStyle -> Large, PlotTheme -> "Detailed"]
which gives
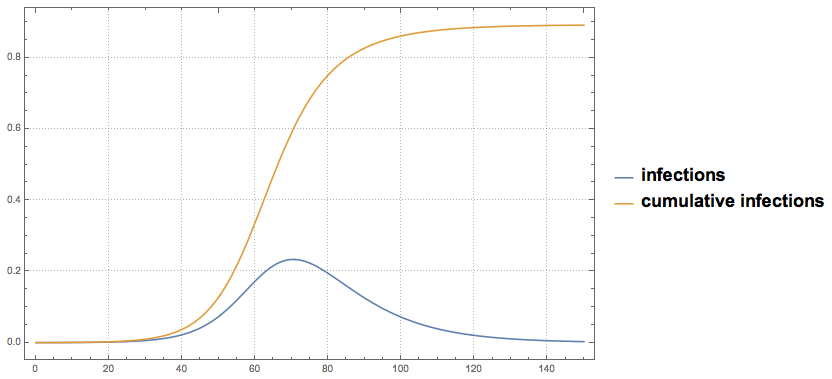 with 0.01% of the population initially infected. Horizontal axis is days while vertical is fraction of initial population.
with 0.01% of the population initially infected. Horizontal axis is days while vertical is fraction of initial population.We see that at the peak of infection, 63% of the population has already been infected, but an additional 26% will become infected for a total of 89% of the population. This implies 0.98% of the population will not recover. For the U.S., this would be roughly 3.3 million deaths. This does not include deaths due to lack of emergency healthcare availability. However, this does represent the trajectory if no actions are taken. Since, is not known precisely, we vary and find
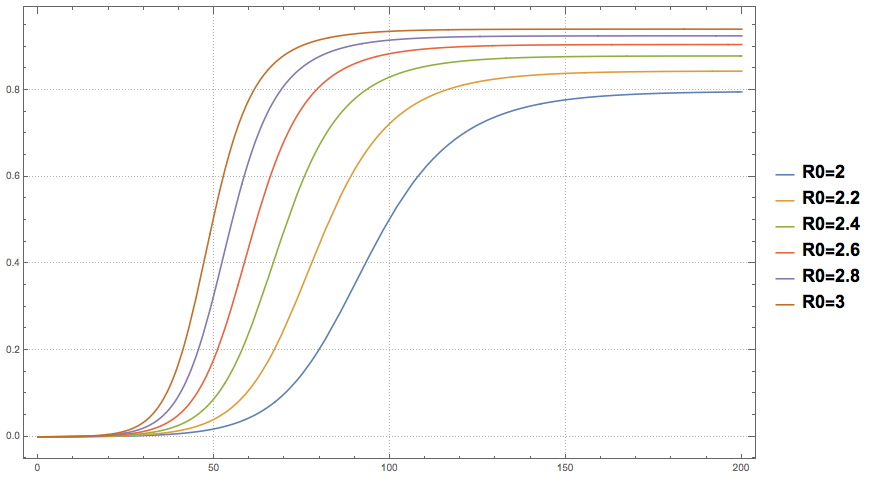 with 0.01% of the population initially infected. Horizontal axis is days while vertical is fraction of initial population that will become infected.
with 0.01% of the population initially infected. Horizontal axis is days while vertical is fraction of initial population that will become infected.So, an optimistic value of  still leads to 80% of the population becoming infected. Regardless of the value of , this represents the natural progression until we reach “herd immunity”. Herd immunity comes at a great cost.
still leads to 80% of the population becoming infected. Regardless of the value of , this represents the natural progression until we reach “herd immunity”. Herd immunity comes at a great cost.
Fortunately, humans can be rational beings. We can affect the math above by individual actions.
In this simplified model, the only term we can directly affect by our actions is the infection rate:
 .
.
New infections will only occur if the infected are allowed to freely mingle with the susceptible population. We can can either quarantine the infected or we can “social distance” so there will be minimum contact between individuals. If there are no contact between susceptible and infected, then  effectively. Of course, not everyone will comply. Let’s assume that 80% of the population does comply with “social distance”, then
effectively. Of course, not everyone will comply. Let’s assume that 80% of the population does comply with “social distance”, then  . Clearly, “social distancing” is a blunt tool, however it’s currently the only tool.
. Clearly, “social distancing” is a blunt tool, however it’s currently the only tool.
So, let us assume that initially and on day 50, some fraction of the total population practice “social distancing”, we then find
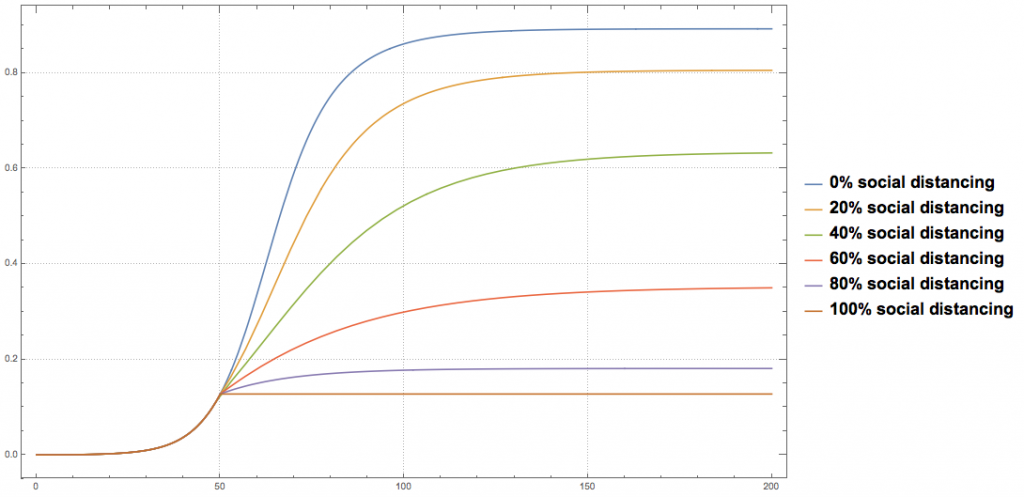
We now see that instead of 89% of the population eventually becoming infected, we can significantly reduce this number if most (>80%) people practice “social distancing”. If 80% comply, then 18% of the initial population will be infected (and equivalently 0.198% deaths or 673 thousand for the U.S.). However, in this case “herd immunity” is never reached and so measures need to be taken to insure  stays below 1.
stays below 1.
How can stay below 1?
Initially, if testing was widely available, then infected individuals could be quarantined and their contacts could be isolated until they either show signs of infections or not (about 14 days since 5.1 days appear to be the mean latency period between becoming exposed and showing symptoms of infection).
Unfortunately, the U.S. appears to have missed this early stage due to lack of testing and tracking.
We can continue the blunt “social distancing”, however this will not insure “herd immunity” and so society, in general, needs to be vigilant. However, at some point, the number of infected will drop and “social distancing” can be relaxed. However, if any “hot spots” develop, then “social distancing” will be needed to once again quench the spread of infections. This does not appear to be a long term solution.
Of course if a vaccine can be developed, then we can simply apply the vaccine to a sufficient number of people so “herd immunity” can be achieved. Given an , then at least  ~ 60% people need to be vaccinated/recovered. We will point out there are many infectious diseases that have no vaccine developed (e.g. HIV). To assume such a vaccine will be available is, perhaps, wishful thinking.
~ 60% people need to be vaccinated/recovered. We will point out there are many infectious diseases that have no vaccine developed (e.g. HIV). To assume such a vaccine will be available is, perhaps, wishful thinking.
Another way to effectively reduce is for every susceptible individual to wear a mask. Clearly, healthcare workers need masks so simple supply arguments say this isn’t feasible. Even if the supply was there, masks are not 100% effective. Most masks we see people wearing are remarkably low at filtering out a virus (~200nm size). Don’t kid yourself, even if everyone wore a mask and they knew the proper procedures, decreases about the same as if only 30% of the population complied with “social distancing” (for those interested, explore “air filter design”). Yes, it helps the individual, but does not stop the increasing rate of infection in the population. Wearing a mask does not excuse you from “social distancing”. Nor does wearing a mask allow us to achieve “herd immunity”. Other solutions are needed.
“Social distancing” is needed because currently there is no way knowing who is infected (or exposed). If we knew who was infected, then we could quarantine those and track who they may have contacted (the exposed) and isolate them also from the general population.
Therefore, it appears to be obvious we need fast and cheap testing for the infection itself (to identify those infected) and those who have recovered and are immune (antibodies detection). The idea here is if you want to stop “social distancing”, then only those not infected or exposed are allowed to freely mingle. Fast testing would help here. Testing also needs to be cheap so that people can be tested regularly as needed. Further, for those who have immunity due from recovery, no restrictions are required for them (assuming they stay immune, of course).
While wide spread testing raises privacy issues, only those currently infected need to be tracked. Safe guards could be put into place to not only protect individuals but society in general.
Tell your representatives to get fast testing up. Tell them to cover the costs so everyone can get tested. Then get tested so we have better information to manage this pandemic. Until then, stay put. Stay away from others (if you can). And check on your neighbors.
This is an extraordinary time. Behave accordingly. It’s for your, mine and other’s best interest.
Add a Comment